- Ruby Hall Clinic, near Wanowrie, Pune, Maharashtra
- Mon - Fri: 9:00 am - 4:00 pm

Gallery Posts






This is a case that I will probably remember throughout my practice. It is special because it is actually a theory coming to reality. It is the case of a 39-year-old female, overweight, who was being treated by her family physician in view of hypertension. Hypertension at such a young age is unusual, and the patient was already on 3 medications to control her blood pressure. The patient reported having fatigue and chest pain on exertion for a very long time (approximately 2 years). She had visited multiple hospitals in the past 2 years but was sent back home, and her symptoms were trivialized. The patient started limiting her activity and was confined most of the time to her house, apart from going to her office for work. The patient is an avid foodie, so she naturally started gaining weight (more calories being credited and no debit in activities, so her bank calorie balance (body weight) was growing!)
The family physician to whom I was recently introduced decided that the patient should see me in view of her long-term symptoms. The patient and her husband came to my OPD, and we had a discussion about her case. In our discussion, I could deduce that although her symptoms were cardiac, they were quite non-specific. We decided to stratify this patient by doing some basic cardiac tests and blood work. In the patient interview, there was a red flag: the patient’s father had a heart attack at 33 years of age, and his paternal grandfather had died in his early forties of a cardiac problem.
During the evaluation, patients’ ECG and 2D echo turned out to be normal (as is the case in most individuals until and unless they have already had a heart attack, then these tests come out to be abnormal). I asked the patient to walk on a treadmill with an ECG hooked up, and to everyone’s surprise, she couldn’t walk for even 2 minutes. My team and I thought of 2 differentials at this stage, the first being de-conditioning, a situation where the body is not used to exertion at all, so a person cannot walk and gets fatigued in 2 minutes, or the most dangerous of all, a blockage in the coronary vessels, the blood vessels that supply the heart.

I counseled the patient and her husband about the need for further investigations, and they were cooperative enough to agree to a CT (coronary angiogram), a simple test that delineates the blood vessels and gives an idea of blockages. The patient visited the facility, and the investigation was done the next day. I got a call from the Radiology Department immediately, as they were in disbelief seeing the images—a young 39-year-old lady with tight blockages in all three blood vessels supplying the heart!
I contacted the husband to come down to the OPD, as it had now become an emergency. Meanwhile, her blood work came up, which showed her LDL cholesterol to be 297 mg/dl (the ideal upper limit is 90). Her condition was akin to a time bomb; it could blow up any minute. As a routine OPD patient, she had become an urgent case!
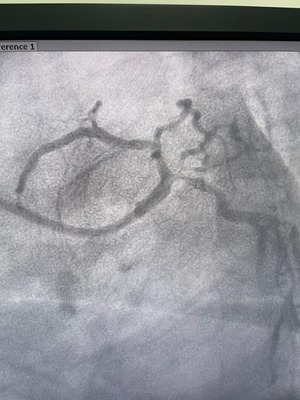
The patient and her husband agreed to an admission, and her insurance company was contacted. Unfortunately, the day of the procedure was a national holiday, so the insurance company was short-staffed, and the approval took an unusually long time. Finally, the patient was up in the cath lab, and the picture of her angiogram was worse than what we anticipated from the CT angiogram! She had blockages in the left main artery along with all the 3 blood vessels. Post-angiogram, I spoke with the relatives and showed them the images. They had 2 options: bypass surgery or a very complex angioplasty. The patient was on the table, her immediate kin was to take the call, and to my surprise, they rejected the idea of bypass surgery at such a young age and trusted me with her life to do an angioplasty!